Herpes Simplex Virus Type 2 Encephalitis in an Immunocompetent Adult: A Diagnostic Challenge
Herpetic encephalitis is the most common cause of fatal sporadic encephalitis. Beyond the neonatal period, herpes simplex virus type 1 (HSV-1) is the etiologic agent in nearly all cases, with < 10% of cases attributable to HSV-2. Nevertheless, neurological infections caused by HSV-2 are responsible for significant morbidity and mortality. Therefore, it must be diagnosed and treated at an early stage. It is classically characterized by a triad of fever, headache, and behavioral changes. The association of these symptoms, laboratory tests, and imaging is fundamental for the early diagnosis and immediate treatment of this pathology to prevent its progression from being fatal. We report a rare case of HSV-2 encephalitis in a previously healthy 61-year-old man, free of genital lesions, who presented with altered mental status, fever, altered cerebrospinal fluid (CFS) with lymphocytic pleocytosis, normal brain imaging, and an initially negative CFS polymerase chain reaction for HSV-1 and HSV-2.
Introduction
Encephalitis is defined as an acute syndrome caused by diffusion and inflammatory. Processes that affect the brain parenchyma, resulting in an altered mental status and various combinations of symptoms that confer an elevated morbidity and mortality rate [1]. This inflammatory process has many causes; it can be infectious, postinfectious, or noninfectious. However, the most common cause is infection due to neurotropic viruses. Enteroviruses, varicella-zoster virus, and herpes simplex virus (HSV) are the most frequent agents. HSV type 1 (HSV-1) is accountable for approximately 90% of the cases seen in adults and children [2]. HSV type 2 (HSV-2) is responsible for 10% of acute viral encephalitis cases in adults, with a predilection to mainly affect immunocompromised patients [3].
This case report addresses the clinical manifestations and diagnostic approach of HSV-2 encephalitis and its management. While this approach is general, we particularly focused on the utility of repeated lumbar punctures and empirical treatment based on the clinical deterioration of the patient in the absence of brain imaging evidence of inflammatory processes.
Case Presentation
A 61-year-old man with an unremarkable medical history was evaluated at the emergency department with a 3 h history of language alterations, including dysarthria, bradylalia, and anomia. He denied having headaches, visual, auditory, coordination, or language alterations. The patient was generally well before admission. He did not use tobacco or illicit drugs and consumed alcohol occasionally. He had engaged in unprotected sexual intercourse three weeks before. On examination, the temperature was 38.4 °C, pulse
108 beats/min, blood pressure 115/70 mmHg, respiratory rate 20breaths/min, and oxygen saturation 97% on room air. He was oriented towards the person, place, and time. General and neurological examinations, including examination of the function of cranial nerves II through XII, were normal. No genital lesions were observed.
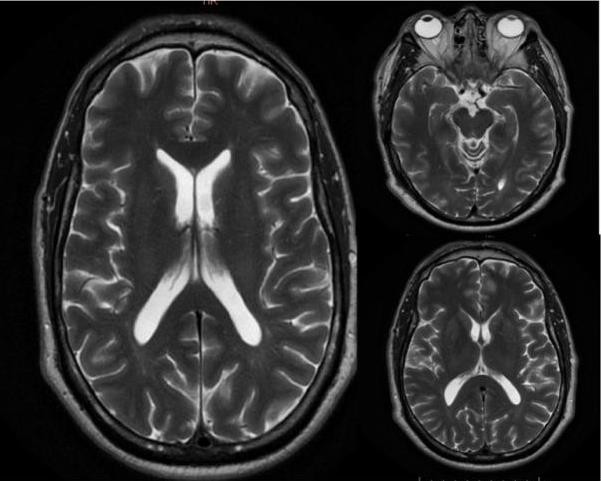
He was admitted to the internal medicine ward to initiate a therapeutic and diagnostic approach. Due to the persistence of his impaired neurological status, gadolinium- enhanced magnetic resonance imaging (MRI) of the brain was performed, which was normal, without any enhancement or anatomical disturbances (Figure 1). Electroencephalography (EEG) revealed no paroxysms, lateralization, epileptiform discharges, or focalization.
A lumbar puncture was requested, which showed hemorrhagic cerebrospinal fluid (CFS) with lymphocytic pleocytosis, increased protein concentrations, and slightly low glucose levels (Table 1). Empirical treatment with ceftriaxone (2 g IV every 12 hours), vancomycin (1 g IV every 12 hours), and acyclovir (10 mg/kg) was initiated. Multiplex polymerase chain reaction (PCR) in CFS was performed, and VHS-1 and VHS-2 were reported as negative.
Three days after admission, neurological deterioration was evident; the patient referred to visual hallucinations, disorientation, and short-term memory disturbances; lumbar puncture was repeated and quantitative viral load for HSV1 and HSV2 was requested, confirming herpetic encephalopathy by HSV2, with a viral load of 2.180 copies/mL (Table 1). The patient was then admitted to the intermediate care unit (ICU) for close monitoring of neurological function as he presented with dysarthria, visual hallucinations, and diminished osteotendinous reflexes.
After six days of ICU stay, the mental status improved, and he persisted without alteration in gnosias, praxias, calculation, judgment, or abstraction. The patient was discharged from the ICU and admitted to the internal medicine floor. He had no fever, but experienced diminished confusion, with some residual forgetfulness and “fogginess”.
A control lumbar puncture was repeated after 14 days of treatment with acyclovir at meningeal doses, and treatment was completed after 21 days with recovery “ad integrum” of the neurological state with a normal EEG.
| DAY 1 | DAY 4 | DAY 14 | REFERENCE RANGE | |
|---|---|---|---|---|
| Color | Hematic | Xantocromic | Clear | Clear |
| Turbidity | Slight | Slight | Clear | Clear |
| Glucose (mg/dL) | 43 | 35 | 60.8 | 45 - 75 |
| Protein (mg/dL) | 378.7 | 141.1 | 178.7 | 15 - 45 |
| Chloride (mmol/L) | 131.1 | 69 | 132 | 118 - 132 |
| WCC (/uL) | 380 | 413 | 60 | |
| Mononuclear (%) | 80% | 88 | 98 | |
| Polymorphonuclear cell (%) | 20% | 12 | 2 | |
| Red cell count (per mm3) | 3.8 | 10.6 | 20 | 0 - 5 |
| Crenocytes | 0 | 0 | ||
| Culture | Negative | Negative | Negative | Negative |
| Molecular panel for meningitis | ||||
| HSV-1 (copies/mL) | - | 0 | 0 | Negative |
| HSV-2 (copies/mL) | - | 2.18 | 0 | Negative |
| Polymerase chain reaction test | ||||
| - E. coli k1 | Negative | Negative | Negative | Negative |
| - Haemophilus influenzae | Negative | Negative | Negative | Negative |
| - Listeria monocytogenes | Negative | Negative | Negative | Negative |
| - N. meningitidis | Negative | Negative | Negative | Negative |
| - S. agalatiae/pneumoniae | Negative | Negative | Negative | Negative |
| - Cytomegalovirus | Negative | Negative | Negative | Negative |
| - Enterovirus | Negative | Negative | Negative | Negative |
| - Varicella Zoster Virus | Negative | Negative | Negative | Negative |
| - Cryptococcus Neoformans | Negative | Negative | Negative | Negative |
| - HSV-1 | Negative | Negative | Negative | Negative |
| - HSV-2 | Negative | Positive | Negative | Negative |
Table 1: Cerebrospinal fluid findings during hospitalization WCC: white blood cell count; HSV-1, herpes simplex virus type 1; HSV
Discussion
HSV infections of the central nervous system (CNS) are among the most severe viral infections of the human brain, and despite available antiviral therapy they represent one of the most devastating infections of the CNS [4]. The diagnosis of viral encephalitis is based on the presence of major criteria, such as altered mental status (level of consciousness, lethargy, or neuropsychiatric disorders) lasting more than 24 h, after ruling out the differential diagnosis [5]. Seizures can occur, and CSF pleocytosis with focal abnormalities on MRI and altered EEG studies are frequently observed.
Both HSV-1 and HSV-2 are double-stranded DNA viruses that belong to the Herpesviridae family; HSV-1 and HSV-2 are closely related with nearly 70% genomic homology. HSV-
2 causes genital herpes, and HSV-1 is typically transmitted during childhood via the orolabial mucocutaneous surfaces and primarily causes herpes labialis [6]. HSV-2 is principally, but not exclusively, acquired through sexual activity, and transmission from male to female partners is more common. It is estimated that 16.2% of all adults between 14 and 49 years have genital herpes [7, 8].
Herpes virus infects mucosal cells, establishing a lifelong latent infection in the innervation of the sensory and autonomic ganglia near the site of infection. In immunocompetent adults, HSV-2 typically causes uncomplicated genital diseases [7]. Primary HSV-2 infection is usually asymptomatic and causes genital herpes in few patients with recurrences, but of those symptomatic with primary genital herpes, 36% of women and 13% of men experience meningeal signs and pleocytosis on CSF examination. HSV-2 encephalitis in adults is extremely rare, accounting for less than 2% of all cases of herpes simplex encephalitis [9].
Viral neurotropism affects glial cells, causing hemorrhagic necrosis mainly in the temporal lobes [7] Host factors, such as age and level of immunocompetence, are the main determinants of the disease, although the variability in the neurovirulence of the herpes virus must also be considered [8]. Although the prognosis of herpes simplex encephalitis has improved dramatically since the availability of antiviral therapy, sequelae in surviving patients can include neurological deficits, seizures, and neuropsychological dysfunctions that greatly impair the quality of life [9]. A delay of 48 h or more at the start of acyclovir treatment is associated with a worse prognosis.
T cell-mediated immunity is essential for HSV control. Therefore, immunosuppressed patients, such as organ transplant recipients receiving chemotherapy, are at increased risk of developing severe opportunistic brain infections [10]. This is particularly important, as newer immunotherapies are being increasingly used to treat autoimmune diseases, malignancies, and other disorders, resulting in an increased risk of infection and atypical manifestations [10]. HSV-2 infection is common in neonates and is caused by transplacental transmission or infection of the birth canal.
It is extremely rare in adult patients and not yet fully understood. However, it may occur in previously healthy patients, as in the present case. The clinical manifestations of HSV encephalitis are variable, but the most common presentations are fever, headache, altered mental status, nausea, vomiting, and neurological deficits, including receptive aphasia, hemiparesis, and seizures.
Laboratory investigations, imaging, and CSF analysis are crucial for the diagnosis of encephalitis [11]. MRI findings may be nonspecific or specific. Hypersensitivity can be observed in the cortical and subcortical regions of the bilateral temporal, frontal, and insular lobes on T2- weighted images (WI). Associated restricted diffusion, gyral swelling, loss of gray-white matter interface, and mild or no enhancement are also observed [12].
HSV 2 infection causes diffuse brain edema, which is seen as hyperintensity on T2WI. Associated diffusion restriction and hemorrhage may also be present [13]. When viral encephalitis is clinically suspected, CSF should be sent for HSV-1 and HSV-2 PCR studies. PCR analysis of the CSF for the detection of HSV DNA has virtually replaced brain biopsy as the gold standard for diagnosis. Schloss, et al. reported that although quantitative PCR is more rational than nested PCR, quantitative PCR has little prognostic use [14].
PCR is highly sensitive (94%-98%) and specific (98%- 100%). Positive results are obtained within 24 h of symptom onset and remain positive for at least 5 to 7 days after the start of antiviral therapy. Although PCR is preferable to brain biopsy, false-negative results can occur early after disease onset [15]. Negative PCR tests are associated with low CSF protein and leukocyte counts; therefore, guidelines recommend repeating CSF HSV-1 PCR testing within 3 to 7 days in highly suspicious cases while continuing empiric therapy [16, 17].
With the suspicion of viral encephalitis, intravenous acyclovir should be initiated empirically as soon as possible to preserve the functionality and life of the patient [16], while the diagnosis is confirmed with the detection of genetic material of the causative virus. Despite effective antiviral therapy, the mortality remains as high as 4%-28%, and only approximately 15%-38% of patients return to a normal level of functioning. Neurological HSV-2 infection can cause monophasic and recurrent aseptic meningitis, which is characterized by self-limited episodes of fever, meningismus, and severe headache. Additionally, myelitis and radiculitis are associated with HSV-2 [18].
Conclusions
HSV is an important human pathogen that is responsible for severe morbidity and mortality. Most HSV-2 encephalitis cases reported in the medical literature are mainly described in immunosuppressed patients, and this case is described in a previously healthy man, free of genital lesions.
This case represents a diagnostic challenge due to initial negative HSV PCR in CFS and normal MRI and EEG, due to which HSV encephalitis diagnoses was seriously questioned; however, the highly suggestive clinical picture and the initial CSF findings consistent with encephalitis, where key elements for continuing antiviral treatment and repeating lumbar puncture with viral load for HSV-1 and HSV-2.
If the clinical suspicion of herpetic encephalitis remains high, treatment should be started as soon as possible, and CSF HSV PCR testing should be performed. However, negative results should be interpreted in the context of the patient’s clinical presentation and the timing of CSF sampling.
Declaration of Interest
None
Acknowledgement
None
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not- for-profit sectors.
References
-
Venkatesan A, Tunkel AR, Bloch KC, Lauring AS, Sejvar J, et al. (2013) Case Definitions, Diagnostic Algorithms, and Priorities in Encephalitis: Consensus Statement of the International Encephalitis Consortium. Clin Infect Dis. 57(8): 1114-1128.
-
Liu FY, Mouhayyar ElC, Mamtani R, Dammann F, Basein T (2020) A case of herpes simplex 2 encephalitis with an unusual radiographic manifestation. IDCases 21: e00884.
-
Aurelius E, Johansson B, Skoldenberg B, Forsgren M (1993) Encephalitis in immunocompetent patients due to herpes simplex virus type 1 or 2 as determined by type-specific polymerase chain reaction and antibody assays of cerebrospinal fluid. J Med Virol 39(3): 179-186.
-
Tyler KL (2018) Acute Viral Encephalitis. N Engl J Med 379(6): 557-566.
-
Whitley RJ (1990) Viral Encephalitis. N Engl J Med 323(4): 242-250.
-
Egan KP, Wu S, Wigdahl B, Jennings SR (2013) Immunological control of herpes simplex virus infections. J Neurovirol 19(4): 328-345.
-
Steiner I, Benninger F (2013) Update on Herpes Virus Infections of the Nervous System. Curr Neurol Neurosci Rep 13(12): 414.
-
Whitley RJ (2006) Herpes simplex encephalitis: adolescents and adults. Antiviral Res 71(2-3): 141-148.
-
Logan SA, MacMahon E (2008) Viral meningitis. BMJ. 336: 36.
-
Tan IL, McArthur JC, Venkatesan A, Nath A (2012) Atypical manifestations and poor outcome of herpes simplex encephalitis in the immunocompromised. Neurology 79(21): 2125-2132.
-
Ellul M, Solomon T (2018) Acute encephalitis - diagnosis and management. Clin Med Lond 18(2): 155-159.
-
Misra UK, Kalita J, Phadke RV, Wadwekar V, Boruah DK, et al. (2010) Usefulness of various MRI sequences in the diagnosis of viral encephalitis. Acta Trop 116(3): 206- 211.
-
Jayaraman K, Rangasami R, Chandrasekharan A (2018) Magnetic Resonance Imaging Findings in Viral Encephalitis: A Pictorial Essay. J Neurosci Rural Pract 9(4): 556-560.
-
Steiner I, Schmutzhard E, Sellner J, Chaudhuri A, Kennedy PG, et al. (2012) EFNS-ENS guidelines for the use of PCR technology for the diagnosis of infections of the nervous system. Eur J Neurol 19(10): 1278-1291.
-
Roberts JI, Jewett GAE, Tellier R, Couillard P, Peters S, et al. (2021) Twice Negative PCR in a Patient With Herpes Simplex Virus Type 1 (HSV-1) Encephalitis. Neurohospitalist 11(1): 66-70.
-
Tunkel AR, Glaser CA, Bloch KC, Sejvar JJ, Marra CM, et al. (2008) The management of encephalitis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis 47(3): 303-327.
-
De Tiege X, Rozenberg F, Burlot K, Gaudelus J, Ponsot G, et al. (2006) Herpes simplex encephalitis: diagnostic problems and late relapse. Dev Med Child Neurol 48(1): 60-63.
-
Saito M, Kiyozaki H, Obitsu T, Imoto H, Taniyama Y, et al. (2016) Herpes simplex virus- 1 encephalitis induced by chemoradiotherapy and steroids in an esophageal cancer patient: a case report. BMC Cancer 16: 233.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia